
Cerebral palsy (sometimes referred to as CP) is a persistent (but not unchanging) disorder of movement, coordination and posture as the result of one or more non-progressive abnormalities in the brain, before its growth and development are complete.
One in 278 children has cerebral palsy.

- 'Cerebral' – means that the cause of the difficulties is in the brain – not in the muscles themselves.
- 'Palsy' – means paralysis.
- 'Persistent' – means that the effects of the brain impairment on movement and posture do not go away. This means that cerebral palsy is a lifelong condition.
- 'Not unchanging' – means that while the condition will always remain, movement patterns may change as the result of development and/or therapeutic intervention, eg physiotherapy.

Although the effects of cerebral palsy are seen in the muscles, it is caused by damage to the part of the brain that controls these muscles – the cerebrum.
The cerebrum is also responsible for other important brain functions, such as communication skills, memory and the ability to learn. This is why some children with cerebral palsy also have learning and communication difficulties.
Damage to the cerebrum can also cause problems with vision and hearing.

In the past, it was thought that the damage to the brain in children with cerebral palsy occurred during difficult or complicated births, as a result of the baby being temporarily deprived of oxygen (asphyxia).
However, a major research project carried out in the 1980s showed that asphyxia was only responsible for an estimated five to ten per cent of cases of cerebral palsy. Most cases occurred as a result of damage to the brain before the child was born.
Although the adult brain is quite adaptable and can recover from quite serious damage, the brains of children, especially during the first six months of development, are particularly vulnerable. Any damage that occurs during this time can have serious and lifelong consequences.

There are three main types of cerebral palsy:
- Spastic – 80% of children with cerebral palsy have this – features include tight muscles, stiff jerky movements, difficulty in moving from one position to another and with holding and releasing objects
- Athetoid – 10% of children with cerebral palsy have this – features include involuntary movements in the face, arms, and trunk
- Ataxic – 5-10% of children with cerebral palsy have this – features include unsteady, wide gait when walking and tremor.
About 10% of children have a mixed-type of cerebral palsy.
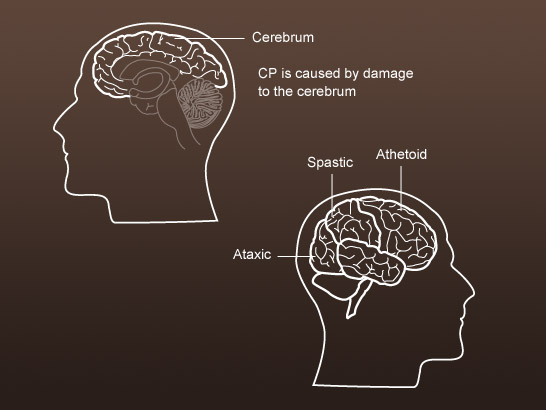
The type of cerebral palsy depends on the area of the cerebrum that is affected.

Children with cerebral palsy may have associated difficulties with:
- Auditory and visual processing
- Sensory sensitivity
- Proprioception, which is the sense knowing where our bodies are in space and in relation to each other, and
- Behaviour associated with their physical and learning needs.

No two children are affected by cerebral palsy in exactly the same way, so individual treatment programmes vary widely. However, all children with cerebral palsy have movement problems so an important component of treatment is likely to be a therapeutic exercise program.

Depending on children's needs a range of professional will work with children with cerebral palsy, most commonly:
- Physiotherapists – focusing on movement
- Occupational therapists – focusing on posture and day-to-day functions, and
- Speech and language therapists – focused on speech, language and eating.
Some special schools build therapeutic programmes into the curriculum. Watch this video clip in which, Tracy, an instructor in communication explains what she is trying to achieve in an oral skills focus group.

The role of speech and language therapists in helping children with eating is less well known than their role in developing speech and language. Watch this video clip in which Sarah, a speech and language therapist, describes her role in relation to feeding. Notice that, although the young man with cerebral palsy featured at the beginning of the video cannot feed himself, using a simple communication aid helps him to take control of what and how much he eats.

Listen to Carolyn, a physiotherapist talking about her role in school. Notice how physiotherapy programmes are built into the school day in special schools.


What could be improved in your own practice to remove barriers for the child? Identify one thing that you could change.
Change it and evaluate the impact on the child's participation and/or learning.