
Cerebral palsy (sometimes referred to as CP) is a persistent (but not unchanging) disorder of movement, coordination and posture as the result of one or more non-progressive abnormalities in the brain, before its growth and development are complete.
One in 278 children has cerebral palsy.

- 'Cerebral' – means that the cause of the difficulties is in the brain – not in the muscles themselves.
- 'Palsy' – means paralysis.
- 'Persistent' – means that the effects of the brain impairment on movement and posture do not go away. This means that cerebral palsy is a lifelong condition
- 'Not unchanging' – means that while the condition will always remain, movement patterns may change as the result of development and/or therapeutic intervention, eg physiotherapy.

Although the effects of cerebral palsy are seen in the muscles, it is caused by damage to the part of the brain that controls these muscles – the cerebrum.
The cerebrum is also responsible for other important brain functions, such as communication skills, memory and the ability to learn. This is why some children with cerebral palsy also have learning and communication difficulties.
Damage to the cerebrum can also cause problems with vision and hearing.

In the past, it was thought that the damage to the brain in children with cerebral palsy occurred during difficult or complicated births, as a result of the baby being temporarily deprived of oxygen (asphyxia).
However, a major research project carried out in the 1980s showed that asphyxia was only responsible for an estimated five to ten per cent of cases of cerebral palsy. Most cases occurred as a result of damage to the brain before the child was born.
Although the adult brain is quite adaptable and can recover from quite serious damage, the brains of children, especially during the first six months of development, are particularly vulnerable. Any damage that occurs during this time can have serious and lifelong consequences.

Researchers believe there are three ways the brain can be damaged before birth:
- Damage to the part of the brain responsible for transmitting signals to the muscles caused by a reduction in the child's blood supply
- Abnormal development of the brain that changes the way it transmits information to the muscles, and
- Bleeding in the child's brain which damages or kills brain tissue.

A few cases of cerebral palsy are caused by damage to the brain that occurs after birth. The damage normally occurs during the first few months of a baby's life, before the brain develops its ability to withstand and adapt to a moderate degree of damage. Damage can be caused by an infection of the brain, such as meningitis, or as the result of a traumatic head injury.

Better maternity care has led to fewer babies being born with cerebral palsy due to birth trauma, however more cases of cerebral palsy are resulting from a much improved survival rate for premature and low birth weight babies. Such babies have a 50% higher risk of cerebral palsy than babies born at full term.
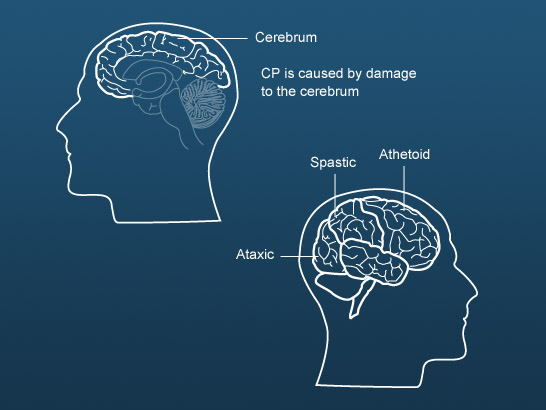
The type of cerebral palsy depends on the area of the cerebrum that is affected.

This is the most common type of cerebral palsy – nearly 80% of all cases.
Children with this type of cerebral palsy may have:
- Tight muscle groups which limit movement
- Stiff and jerky movements
- Difficulty moving from one position to another, and
- Difficulty with holding and letting go of objects.

Spastic cerebral palsy can affect:
- One side of the body effected, usually the arm (hemiplegia)
- Two limbs, the legs are usually affected more than the arms (diplegia), or
- All four limbs, usually the trunk and the muscles that control the mouth, tongue and pharynx (quadriplegia).

This form of cerebral palsy, which affects five to ten per cent of children diagnosed with cerebral palsy, affects balance and depth perception.
Children with ataxic cerebral palsy have poor muscle tone and coordination.
They may:
- Walk unsteadily with a wide based gait, and
- Tremor, especially when they are trying to hold small objects, eg writing implements.

About 10% of children with cerebral palsy have a mixed-type cerebral palsy.
These children have:
- the tight muscle tone of spastic cerebral palsy, and
- the involuntary movements of athetoid cerebral palsy.
This is because they have injuries to both the pyramidal and extrapyramidal areas of the brain. Usually the spasticity is more obvious at first, with involuntary movements increasing when the child is between nine months and three years old.

Some children with cerebral palsy have difficulties with proprioception which is the sense knowing where our bodies are in space and in relation to each other without looking.
Behaviours associated with this may include:
- Clumsiness
- Running but finding walking difficult
- Invading others' space
- Sprawling
- Fidgeting, or
- Stomping about.

Some children with cerebral palsy may exhibit behaviour difficulties associated with their physical and learning difficulties, including, for example they may:
- Not want to get out of bed in the morning
- Refuse to try new things or change form one thing to another
- Not want to join in
- Feel angry easily, and
- Develop uncontrollable fears of normally unthreatening objects, smells, touch or situations.

- Constipation
- Difficulties with sleeping
- Oro-muscular difficulties – chewing, swallowing, speech production
- Epilepsy, and
- Learning difficulties.

No two children are affected by cerebral palsy in exactly the same way, so individual treatment programmes vary widely. However, all children with cerebral palsy have movement problems so an important component of treatment is likely to be a therapeutic exercise program.

Depending on children's needs a range of professionals will work with children with cerebral palsy, most commonly:
- Physiotherapists – focusing on movement
- Occupational therapists – focusing on posture and day-to-day functions, and
- Speech and language therapists – focused on speech, language and eating.
Some special schools build therapeutic programmes into the curriculum. Watch this video clip in which, Tracy, an instructor in communication explains what she is trying to achieve in an oral skills focus group.

The role of speech and language therapists in helping children with eating is less well known than their role in developing speech and language. Watch this video clip in which Sarah, a speech and language therapist, describes her role in relation to feeding. Notice that although the young man with cerebral palsy featured at the beginning of the video cannot feed himself, using a simple communication aid helps him to take control of what and how much he eats.

Listen to Carolyn, a physiotherapist talking about her role in school. Notice how physiotherapy programmes are built into the school day in special schools.

As has already been discussed earlier in this module, neuroplasticity can allow the neurons in the brain to compensate for injury and disease and to adjust their activities in response to new situations or to changes in their environment.
Listen to this audio clip in which Nigel Carter, from MOVE Europe, describes research which indicates that repetitive movement patterns as part of physical therapy can re-pathway or create new neural pathways around brain lesions.


Lead some staff development to introduce colleagues to the research on the neurological basis of cerebral palsy. You may wish to read around the subject a little more widely to inform your planning.
The purpose of this staff development is to raise questions, identify issues and start a dialogue as the first step to auditing and developing practice across the school (Level D). If you can, involve other professionals who work with children with dyscalculia to participate and contribute to the discussion.
Make a list of the questions/issues raised by the discussions.