
Foetal alcohol spectrum disorder (FASD) is the most common preventable cause of learning disability/difficulty in the UK It is caused by heavy maternal alcohol consumption in early pregnancy, either chronic daily use or binge drinking. A number of factors may exacerbate the effects of alcohol, including:
- The pattern and timing of alcohol consumption
- The stage of foetal development, and
- Social behavioural factors, eg poverty and smoking.
Listen to Ali, the adoptive mother of Jade, a child with FAS, as she explains what FAS is. Notice the variability of the FAS population.


It is estimated that that the current prevalence of FASD in populations of younger school children may be as high as two to five per cent in the USA and some western European countries (May et al, 2009).
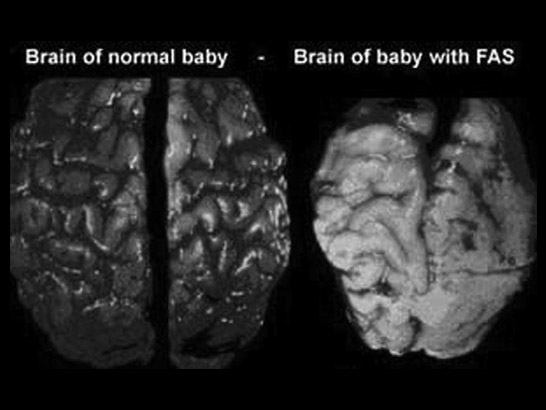
Brain damage is the most serious aspect of FASD. This damage is permanent. It can be accommodated but not reversed. Look at this image. It shows an example of extreme alcohol damage to the brain of a baby with FAS. As with this baby, those who have this degree of damage are unlikely to survive into infancy.

The developmental profile of children with FASD is variable. Expressive language may be in advance of their actual age and their reading skills may be chronologically appropriate. In areas such as social skills and emotional maturity they may be performing at half their developmental age.
Mathematical and numerical concepts are particularly challenging for these children in that, for some, the parietal lobe of the brain, which controls numeracy and computational activity in the brain may have significantly reduced functioning.
Listen to Ali, Jade's mother, again. This time she talks about Jade's 'spiky profile'. Jade has high cognitive skills but her affective skills (skills in emotional areas) and her ability to cope with everyday life are similar to those found in a much younger child.


Listen to the short audio clips on the next slide in which Ali talks about Jade's difficulties at school.
Using the list on the previous screen and information from the audio clip, consider how you would respond to having a child with FAS in your classroom. What approaches might work best for each of the learning needs identified above?
Compare your answers with the findings from Carpenter's research on the next screen.
-
 Jade clip 11:24
Jade clip 11:24 -
 Jade clip 21:38
Jade clip 21:38 -
 Jade clip 31:53
Jade clip 31:53

May, P., Gossage, J., Kalberg, W., Robinson, L., Buckley, D., Manning, M. and Hoyme, E. (2009) Prevalence and epidemiologic characteristics of FASD from various research methods with an emphasis on recent in-school studies, Developmental Disabilities Research Review, 15 (3), 176-192
Blackburn, C., Carpenter, B. and Egerton, J. (2012), Educating children and young people with Foetal Alcohol Spectrum Disorders: Constructing personalised pathways to learning, Routledge.
Blackburn, C. (2010) Facing the challenge and shaping the future for primary and secondary aged students with Foetal Alcohol Spectrum Disorders (FAS-eD Project). London: NOFAS-UK.
Blackburn, C., Carpenter, B. and Egerton, J. (2010) Shaping the future for children with foetal alcohol spectrum disorders. Support for Learning, 25 (3), 139-145.
British Medical Association (2007) Foetal Alcohol Spectrum Disorders: A guide for healthcare professionals. London: British Medical Association.
Carpenter, B. (2011) Pedagogically bereft! Improving learning outcomes for children with foetal alcohol spectrum disorders. British Journal of Special Education, Vol 38, No 1 pp37 – 43.
Clarren, S. (2004) Teaching Students with FASD. Alberta, Canada: Alberta Learning.